Tutorials
Top sites for Diabetes |
TUTORIAL 4: COMPLICATIONS OF TYPE 2 DIABETES
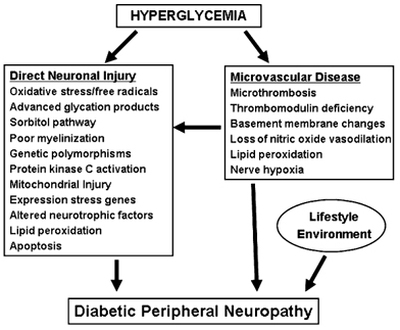
Without tight control of blood glucose levels, type 2 diabetes can lead to a wide range of serious complications that can be life-threatening. These complications can be further exacerbated by high blood pressure, elevated cholesterol levels and obesity. ______________________________________________________________________________________________________________________________________ Hyperosmolar Hyperglycaemic State (HHS) Type of diabetic coma associated with a high mortality seen in diabetes mellitus type 2. Also known as hyperosmotic non-ketotic coma (HONK). It is called hyperosmolar hyperglycemic state (HHS) because some patients may have some ketonuria and it does not necessarily cause coma. Usually precipitated by an infection, myocardial infarction, stroke or another acute illness. Extremely high (above 300 mg/dl (16 mmol/L)) blood glucose levels lead to water being osmotically drawn out of cells into the blood causing the kidneys to eventually begin excreting glucose into the urine. This results in loss of water and an increase in blood osmolarity. If fluid is not replaced (by mouth or intravenously), the osmotic effect of high glucose levels, combined with the loss of water, will eventually lead to dehydration. The body's cells become progressively dehydrated as water is taken from them and excreted. Electrolyte imbalances are also common and are always dangerous. Urgent medical treatment is necessary, commonly beginning with fluid volume replacement. The increasing hemoconcentration and volume depletion may result in: Hyperviscosity and increased risk of thrombosis, disordered mental functioning, focal neurological impairment and ultimately can cause death. ______________________________________________________________________________________________________________________________________ Chronic elevation of blood glucose level leads to damage of blood vessels. The endothelial cells lining the blood vessels take in more glucose than normal, since they do not depend on insulin. They then form more surface glycoproteins than normal, and cause the basement membrane to grow thicker and weaker. In diabetes, the resulting problems are grouped under "microvascular disease" (due to damage to small blood vessels) and "macrovascular disease" (due to damage to the arteries). ______________________________________________________________________________________________________________________________________ Macrovascular Complications >Coronary artery disease, leading to angina or myocardial infarction ("heart attack") >Diabetic myonecrosis ('muscle wasting') >Peripheral vascular disease, which contributes to intermittent claudication (exertion-related leg and foot pain) as well as diabetic foot. >Stroke (mainly the ischemic type) >Diabetic Foot: often due to a combination of sensory neuropathy (numbness or insensitivity) and vascular damage, increases rates of skin ulcers (diabetic foot ulcers) and infection and, in serious cases, necrosis and gangrene. It is why diabetics are prone to leg and foot infections and why it takes longer for them to heal from leg and foot wounds. It is the most common cause of non-traumatic adult amputation, usually of toes and or feet, in the developed world ______________________________________________________________________________________________________________________________________ Microvascular Complications The most common microvascular complications of diabetes include: > Diabetic nephropathy, damage to the kidney which can lead to chronic renal failure, eventually requiring dialysis. Diabetes mellitus is the most common cause of adult kidney failure worldwide in the developed world. The earliest detectable change in the course of diabetic nephropathy is a thickening in the glomerulus. At this stage, the kidney may leak more serum albumin (plasma protein) than normal in the urine (albuminuria), and this can be detected by sensitive medical tests for albumin. This stage is called "microalbuminuria". As diabetic nephropathy progresses, increasing numbers of glomeruli are destroyed by progressive nodular glomerulosclerosis. Consequently, urine albumin increases to the point that it may be detected by ordinary urinalysis techniques. At this stage, a kidney biopsy generally clearly shows diabetic nephropathy. > Diabetic neuropathy, abnormal and decreased sensation, usually in a 'glove and stocking' distribution starting with the feet but potentially in other nerves, later often fingers and hands. When combined with damaged blood vessels this can lead to diabetic foot. Other forms of diabetic neuropathy may present as mononeuritis or autonomic neuropathy. These conditions are thought to result from diabetic microvascular injury involving small blood vessels that supply nerves (vasa nervorum) in addition to macrovascular conditions that can culminate in diabetic neuropathy. Relatively common conditions which may be associated with diabetic neuropathy include third nerve palsy; mononeuropathy; mononeuropathy multiplex; diabetic amyotrophy; a painful polyneuropathy; autonomic neuropathy; and thoracoabdominal neuropathy. |
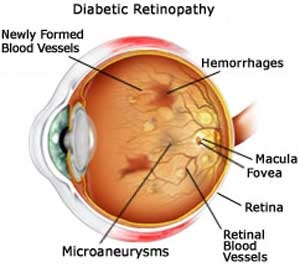
> Diabetic retinopathy: growth of poor-quality new blood vessels in the retina as well as macular edema (swelling of the macula), which can lead to severe vision loss or blindness. Diabetic retinopathy is the result of microvascular retinal changes. Hyperglycemia-induced intramural pericyte death and thickening of the basement membrane lead to incompetence of the vascular walls. These damages change the formation of the blood-retinal barrier and also make the retinal blood vessels become more permeable.